
In the wake of a global pandemic that pushed Canada’s healthcare infrastructure to its breaking point, a new battleground has emerged in the fight for the future of Medicare vs healthcare privatization. The post-pandemic landscape is defined by a brutal reality: severe health worker shortages, physician attrition, and surgical backlogs that stretch for months. In this climate of urgency, the Alberta government has introduced Bill 11—a legislative overhaul framed as “innovation” but seen by investigative analysts and healthcare advocates as a strategic dismantling of the single-payer model.
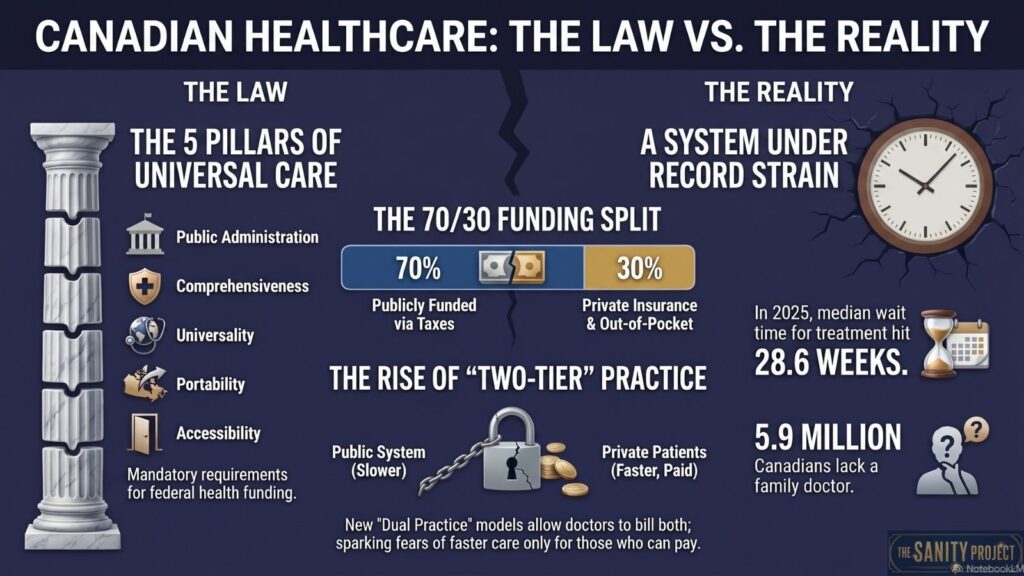
Central to this conflict is the introduction of “dual practice,” a policy that would allow physicians to operate concurrently in both the public and private systems. Organizations such as Canadian Doctors for Medicare (CDM) have warned that this is not a supplementary measure, but a predatory one. By allowing doctors to charge patients privately for faster access while remaining tethered to public funding, Bill 11 threatens to dissolve the social solidarity that defines Canadian healthcare. This is a pivotal choice: do we repair the public foundation or shift toward a U.S.-style, market-driven system where the length of your wallet determines the speed of your care?
The Dual Practice Dilemma: Understanding the Structural Shift in Alberta
The restructuring of healthcare financing in Alberta represents a “decisive shift” away from traditional Medicare. Historically, the Canada Health Act has relied on a clear boundary between public necessity and private luxury. Bill 11 erases that line, creating a legislative environment in which medically necessary care is no longer the exclusive domain of the public single-payer system but a commodity to be sold to the highest bidder.
The “Flexibility” Trap: How Bill 11 Institutionalizes Double-Dipping
Under the proposed framework, Alberta is introducing the “flexibly participating physician.” This is a radical departure from the “opt-out” models found in other provinces (excluding Ontario). In a standard opt-out system, a physician must leave the public system entirely to charge market rates—a high-risk financial move that keeps the public and private pools distinct.
Bill 11 removes this risk, institutionalizing a model of “double-dipping.” Physicians can now bill the public insurance plan for most of their patients while privately billing others for the same medically necessary services. Most critically, Alberta is the first province to explicitly encourage a duplicative private health insurance (PHI) market. This is designed to create a parallel tier of “queue-jumping insurance,” allowing those with private coverage to bypass the very wait times that the public system is struggling to manage.

The Physician Drain: Why Private Incentives Worsen Public Access
The “So What?” of this policy is a grim, zero-sum game for human resources. In a province like Alberta, where there are only 2.4 physicians per 1,000 people—nearly half the ratio of European models like Germany (4.58)—healthcare is a limited resource. Every hour a specialist spends in a private surgical suite is an hour stolen from the public queue.
The financial incentives are staggering. Specialist physicians in Alberta are already compensated at world-class levels, averaging USD $427,795 annually—far exceeding the USD $331,008 earned by their counterparts in Germany. Dr. Thara Kumar, an emergency physician, argues that the ability to earn even more in the private sector for the same care will inevitably create a vacuum. When doctors can earn higher margins from private payers, the public system loses its most valuable asset: time. This does not add capacity; it merely redistributes it toward those who can pay, leaving the public system to manage a shrinking pool of providers and an ever-growing list of patients.
Fact-Checking the Global Benchmarks: The “European Model” vs. Reality
Policy proponents often use “drive-by” international comparisons to justify privatization, pointing to “top-performing” European systems. However, as an investigative analysis reveals, these comparisons are often stripped of their regulatory context to sell a specific narrative.
The Myth of the European Queue-Jumper
While Germany, France, and the Netherlands use private elements, they are fundamentally different from the Alberta model. In Germany, private insurance is an “alternative” to the public scheme, primarily for high-income earners; once you opt out, returning to the public system is notoriously difficult. In France, private insurance is “complementary,” covering co-payments rather than providing a “fast pass” to surgery.
Furthermore, these mixed systems are administratively bloated. France faces management costs accounting for 6% of its total health spending—the second-highest in the OECD—largely due to the complexity of regulating the public-private mix. Unlike the “flexibility” promised in Alberta, European physicians are often salaried employees with strict contractual limits on their private work, ensuring the public core remains the priority.
Subscribe To Our Newsletter!
Lessons from Australia: A Cautionary Tale of Parallel Tiers
The closest global comparison to Bill 11 is Australia, which serves as a stark warning. Australia maintains a parallel private tier supported by massive public intervention. In 2025, the Australian government provided $7.6 billion in tax subsidies to prop up the private insurance industry. Unlike the voluntary model proposed in Alberta, Australia’s system is coercive: high-income individuals face financial penalties if they do not purchase private insurance.
Evidence from Australia shows that this has failed to reduce public wait times. Stephen Duckett, former CEO of Alberta Health Services, notes that the private tier primarily serves to increase physician incomes and investor profits. It has created a system in which the public is taxed to subsidize a private escape hatch that does nothing to alleviate pressure on the general hospital system.
Data Synthesis: Comparative Wait Times for Priority Procedures
The data shows that even with a robust private tier, Australia’s public system wait times are frequently longer than Canada’s current public-only benchmarks.
| Procedure | Australia (Public System Median Days) | Canada (Public System Median Days) |
| Cataract surgery | 118 | 66 |
| Coronary artery bypass graft | 19 | 8 |
| Hip replacement | 135 | 131 |
| Knee replacement | 265 | 161 |
Source: OECD Health Statistics 2023.
While the political debate often fixates on “queue-jumping” for major surgeries, the data reveals a deeper crisis. The focus on surgical privatization distracts from the fact that the public system’s actual “breaking point” is not in the operating room, but in the foundational sectors of primary and mental health care.
The Evidence-Based Path Forward: Quality, Equity, and System Capacity
Evidence-based “Public Solutions” are strategically superior to privatization because they address the root causes of system inefficiency without compromising the “Quadruple Aim”—enhancing patient experience, provider satisfaction, population health, and value for money.
The High Cost of User Fees and Out-of-Pocket Payments
The “So What?” of user fees is a lesson in failed economics. Findings from the McMaster Health Forum and the RAND Health Insurance Experiment prove that out-of-pocket costs deter patients from seeking both “unnecessary” and “essential” care. In a Quebec study, when seniors and welfare recipients were hit with prescription fees, “patient non-adherence” spiked. This led to a surge in emergency department visits and adverse health events. User fees do not save the system money; they simply shift the cost from the pharmacy counter to the much more expensive acute-care hospital bed.

Bridging the Gaps in Primary and Mental Health Care
The true measure of a health system’s health is accessibility. CIHI (2025) data shows that while 83% of Canadians have a regular provider, only 27% can secure a same-day or next-day appointment. The crisis is even more acute in mental health, where 41% of adults report unmet needs.
Public-sector innovation, rather than private equity, offers the path forward. “Integrated Youth Services” (IYS) has shown how public investment can work; in just one year, four provinces saw a 28% increase in youth access to mental health and substance use support through this model. This is a viable public alternative to the fragmented, profit-driven clinics incentivized by Bill 11.
Protecting the Foundation: Strong Public Investment vs. Private Equity
Canada operates on a “National Health Insurance” model (publicly funded, privately delivered by non-profits/small businesses), distinct from the “National Health Service” model (government-owned hospitals) of the UK. Paradoxically, Canada already has a higher share of private financing than many of the European systems it is told to emulate.
Share of Public vs. Private Health Care Financing (2022)
| Jurisdiction | Public Financing | Private Financing (Insurance + Out-of-Pocket) |
| Alberta | 70% | 30% |
| Canada | 71% | 29% |
| Australia | 73% | 27% |
| United Kingdom | 82% | 18% |
| Germany | 87% | 13% |
Source: Figure 3, CCPA Analysis of CIHI and OECD Data.
As Dr. Bernard Ho emphasizes, the solutions to our wait times are found in multidisciplinary teams, centralized referral systems, and robust public investment. Bill 11 departs from social solidarity, choosing to fragment the system for the benefit of private equity and investor-owned delivery. To save the system, we must fix the public foundation, not build a private escape hatch for the few.
——————————————————————————–
The final verdict on Bill 11 is clear: privatization and dual practice do not add capacity; they cannibalize it. Strengthening Canadian healthcare requires doubling down on public investment and innovation, rather than drawing resources away from the public core to serve a market-driven tier.
Listen to the full episode on our podcast at podcast.thesanity.org











